AI: Could it help prevent blindness in diabetics?

2024-12-17 03:02:37
 Dean Raper
Dean RaperThis is the second feature in a six-part series that is looking at how AI is changing medical research and treatments.
Terry Quinn was only in his teens when he was diagnosed with diabetes. In some ways he rebelled against the label and frequent tests, not wanting to feel different.
His biggest fear was of someday needing to have his foot amputated. Vision loss, another possible complication of diabetes, wasn’t really on his radar. “I never thought I’d lose my sight,” says Quinn, who lives in West Yorkshire.
But one day he noticed bleeding in his eye. Doctors told him he had diabetic retinopathy: diabetes-related damage to blood vessels in the retinas. This required laser treatments and then injections.
Eventually the treatments weren’t enough to prevent the deterioration of his vision. He would hurt his shoulder walking into lampposts. He couldn’t make out his son’s face. And he had to give up driving.
“I felt pathetic. I felt like this shadow of a man that couldn’t do anything,” he remembers.
One thing that helped him climb out of his despair was the support of the Guide Dogs for the Blind Association, which connected him with a black Labrador named Spencer. “He saved my life,” says Quinn, who is now a fundraiser for Guide Dogs.
In the UK the NHS invites patients for diabetic eye screening every one or two years.
US guidelines are that every adult with type 2 diabetes should be screened at diagnosis of diabetes, and then annually if there are no issues. Yet for many people, that doesn’t happen in practice.
“There’s very clear evidence that screening prevents vision loss,” says Roomasa Channa, a retina specialist at the University of Wisconsin-Madison in the US.
In the US barriers include cost, communication and convenience. Dr Channa believes that making the tests easier to access would help patients.
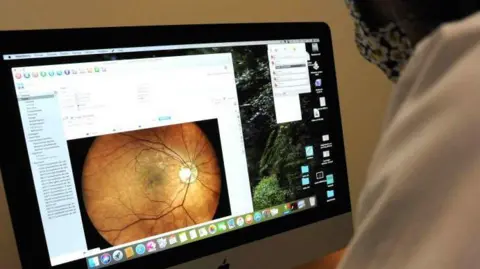
To screen for diabetic retinopathy health professionals take pictures of the rear interior wall of the eye, known as the fundus.
Currently, interpreting fundus images manually is “a lot of repetitive work”, Dr Channa says.
But some think that artificial intelligence (AI) could speed up the process and make it cheaper.
Diabetic retinopathy develops in fairly clear stages, which means that AI can be trained to pick it up.
In some cases, AI could decide whether a referral to an eye specialist is needed, or work in tandem with human image graders.
 Getty Images
Getty ImagesOne such system was developed by the health technology company Retmarker, based in Portugal.
Its system identifies fundus images that could be problematic and sends them to a human expert for further investigation.
“Normally we use it more as a support tool to give information to the human to make a decision,” says João Diogo Ramos, Retmarker’s chief executive.
He believes that fear of change is limiting the take-up of AI-powered diagnostic tools like this.
Independent studies have suggested that systems like Retmarker Screening and Eyenuk’s EyeArt have acceptable rates of sensitivity and specificity.
Sensitivity is how good a test is at detecting disease, while specificity is how good it is at detecting the absence of disease.
In general, very high sensitivity could be linked to more false positives. False positives create both anxiety and expense, as they lead to unnecessary specialist visits. In general, poor-quality images can lead to false positives in AI systems.
 Getty Images
Getty ImagesGoogle Health researchers have been examining the weaknesses of an AI system they developed to detect diabetic retinopathy.
It performed very differently when trialled in Thailand, compared to hypothetical scenarios.
One problem is that the algorithm required pristine fundus images. This was a far cry from the realities of occasionally dirty lenses, unpredictable lighting, and camera operators with different levels of training.
Researchers say they have learned lessons about the importance of working with better data and consulting a wide range of people.
Google is confident enough in its model that in October, the company announced that it was licensing it to partners in Thailand and India. Google also said that it was working with the Thai Ministry of Public Health to assess the cost-effectiveness of the tool.

Cost is a very important aspect of the new technology.
Mr Ramos says that Retmarker’s service could cost around €5 per screening, though with variations according to volume and location. In the US, medical billing codes are set considerably higher.
In Singapore, Daniel S W Ting and colleagues compared the costs of three models of diabetic retinopathy screening.
The most expensive was human assessment. However, full automation was not the cheapest, because it had more false positives.
The most affordable was a hybrid model, where the initial filtering of results was performed by AI, before humans took over.
This model has now been integrated into the Singapore Health Service’s national IT platform and will be going live in 2025.
However, Prof Ting believes that Singapore has been able to achieve cost savings because it already had robust infrastructure for diabetic retinopathy screening.
 Bilal Mateen
Bilal MateenSo the cost-effectiveness is likely to vary greatly.
Bilal Mateen, the chief AI officer at the health NGO PATH, says that the cost-effectiveness data around AI tools to preserve eyesight has been fairly strong in rich countries like the UK, or a few middle-income countries like China. But that isn’t the case for the rest of the world.
“With the rapid advances in what AI is capable of doing, we need to ask less if it’s possible, but more and more whether we’re building for everyone or just the privileged few. We need more than just effectiveness data for effective decision-making,” Dr Mateen urges.
Dr Channa points to the health equity gap even within the US, which she hopes that this tech can help bridge. “We do need to expand it to places that have even more limited access to eye care.”
She also stresses that older people and people with vision problems should see eye doctors, and the convenience of AI for routinely detecting diabetic eye disease should not deter attention to all the other eye diseases. Other eye conditions, like myopia and glaucoma, have proven tougher for AI algorithms to detect.
But even with those caveats, “the technology is very exciting,” says Dr Channa.
“I would love to see all our patients with diabetes screened in a timely fashion. And I think given the burden of diabetes, this is a really potentially great solution.”
Back in Yorkshire, Mr Quinn certainly hopes the new tech takes off.
If AI had existed for earlier detection of his diabetic retinopathy, “I’d have grabbed it with both hands.”